The
Homeopathic Hospital
at Neuilly in France, 1914-1916
by Dr M. Geoffrey Miller.
Presented by
Sylvain Cazalet(Excerpted
from: The Anglo French-American Hospital: An Account of the Work
Carried On Under Homeopathic Auspices during 1915-16 at the Hôpital
Militaire Auxiliare, No. 307, Neuilly-sur-Seine, In Conjunction With the
French Red Cross Society, (Part IV). With Financial Statement,
Medical Report, List of Subscribers’, and Appendices I-VIII. By the
British Committee sitting at London (1917[?])
Editor’s
Note:
Homeopathy
(or Homoeopathy) is the treatment of disease by drugs that in a healthy
person would produce symptoms of that disease. It was widely practiced
during WWI because orthodox management of disease had the capacity to
cause iatrogenic illness as a result of the toxic effects of the drugs
that were commonly prescribed and were not particularly effective in any
case.It
would be true to say that very few medications were truly effective,
certainly not in the way that modern medications are today. There was no
specific treatment for pneumonia, tuberculosis, angina pectoris,
bacterial infections nor a host of illnesses that can now be
significantly improved by medication. A glance at the list of diseases
treated by the Anglo-French Homeopathic Hospital reveals that nearly all
the medical complaints were incurable by the orthodox treatments of the
time and all would fare as well as they would if they were admitted to
the orthodox General Hospitals. Many would do better because of care
that they were given by the dedicated nurses and doctors. These doctors
were all trained in orthodox medicine and knew when to treat by
Homeopathic principles and when to treat by standard methods.The
Hospital was opened at Neuilly in late 1914 and was disbanded on 15th.
March, 1916 because so many of their staff were called up for military
service in the RAMC. During its existence many surgical patients were
treated in their operating room as well as medical patients; the
Hospital had a particular interest in the care of indigent civilians as
well as military patients.
THE HOMEOPATHIC
HOSPITAL AT NEUILLY IN FRANCERAISON D’ETRE OF THE
HOMEOPATHIC HOSPITAL.
EARLY
in the course of the great war, whilst the arrangements – later
perfected – for the sick and wounded were in the making, it became known
that the call for the reception of surgical cases was so considerable
and insistent as to relegate any elaborate provision for the inevitable
medical casualties to a second place.The
first winter –like the Crimean winter– indicated the necessity for an
amplified hospital service for medical cases also. A number of auxiliary
institutions for the wounded had been established in Franco-Belgium,
while medical cases were steadily rising in number. In the circumstances
it seemed hardly possible for Homoeopathy, as a public service, to rule
itself out from that volume of auxiliary hospital establishment which
private initiative was zealously creating.In
the threefold activities of medicine-prevention, the treatment of acute,
and the alleviation of chronic disease-Homoeopathy has a special title
to take a definite position. In the last century it had won its spurs at
a time of public crisis-the first cholera epidemic-by opening the doors
of the London Homoeopathic Hospital to the free admission of cholera
cases, and carrying out homoeopathic treatment so successfully as to
obtain special Parliamentary attention to its high standard of success.
Before that time, on the Continent, where critical comparison was made
between the old school and the new school results in the treatment of
pneumonia, the honours of the time again fell to Homoeopathy. That this
school of therapeutics maintained its powers unabated was evident by the
published results of the London Homoeopathic Hospital in such diseases
of daily life as pneumonia and acute rheumatism. Here again in a
statistical comparison with results of treatment in other institutions,
the issues brought about by Homoeopathy were so striking as to merit the
attention of public bodies. Therefore it was with some past experience –
and some consciousness of special fitness that the project was evolved
of a homoeopathic hospital for medical cases as near as possible to the
scene of warfare.THE DESIGN INTERNATIONAL, THE ORGANISATION
BRITISH.At
a meeting of the Acting Committee of the International Homoeopathic
Council held in London late in 1914, its deliberations included a
proposition for the establishment of a Homoeopathic Hospital, under
military control, for medical cases, on the Western front of the Allies.
Dr G. Burford
Mr. Robert
Henryson CAIRD, J.P.The
President of the British Homoeopathic Society (Dr. Wynne Thomas), the
President of the previous British Homoeopathic Congress (Dr. James
Johnstone), together with the Vice-President of the International
Homoeopathic Council (Dr. George Henry Burford 1856-1937), met by arrangement the
Chairman of the London Homoeopathic Hospital, R. H. Caird, Esq., J.P.,
to consider the necessary preliminaries. Their consultation issued in
the nomination of a Provisional Committee constituted by representatives
of the principal homoeopathic activities in Great Britain, and the
publication of a statement of the case, with an appeal for funds to
those favourably inclined to the work. Thus did the leaders of British
Homoeopathy lead, and the response of the English-speaking homoeopaths
the world over was immediate and maintained. Fortified by this support,
the Provisional Committee nominated two Commissioners (Dr. Hoyle and Dr.
MacNish) to proceed to France to confer with the military authorities
there, as well as with the principal homoeopathic physicians in Paris.
As the issue of this investigation, the Committee decided to work under
the auspices of the French Red Cross Society, and to internationalism as
far as possible, the interest it was desirable to arouse of homoeopathic
supporters in this special procedure.

THE LOCATION OF THE HOSPITAL AT NEUILLY.
The
instructions of the Commissioners had included, as requirements, that
the Hospital be as near as possible to the fighting line, while
retaining easy communication with England as the necessary base for
staff and supplies. The Franco-Belgian area, and the district served by
the Calais-Paris railway were especially noted for investigation ad hoc.
After a primary visit and report the Commissioners made a second
journey, and concluded that Paris itself offered indubitably the maximum
advantages for the location of the proposed Hospital. In this survey the
Commissioners had the profit of the counsel and personal co-operation of
Dr. Bernard Arnulphy of Paris, whose intimate knowledge of localities
and their possibilities was of special and particular value in the
enquiry. The Commissioners further reported, and their report carried
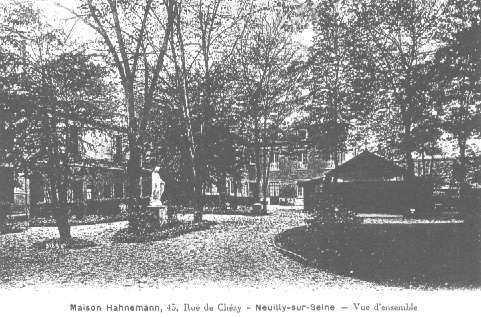
Dr. Arnulphy’s concurrence, that the Villa Borghese at
Neuilly-sur-Seine, already furnished as a large Sanatorium, was
especially suitable alike in location, size, ease of access and general
fitness for the institution proposed by the Committee. Other alternative
sites and buildings were also reported on, but inquiry proved that none
of these was so suitable.

THE NEUILLY HOSPITAL.
Beautiful
for situation, the Villa Borghese, selected by the Board of Management
as the most fitting for the establishment of the Anglo-French-American
Hospital, was an up-to-date modern building, standing in its own grounds
of about 5,000 square metres, in the well-known suburb of Paris,
Neuilly-sur-Seine. The Villa consisted of the original building, with
large entrance hall, ante-rooms, and spacious salons on the ground
floor, each capable of accommodating eight or ten beds and suites of
smaller apartments with bath-rooms on the floors above. The Annexe, an
erection of more recent date and connected with the main building by a
closed-in corridor, contained suites of rooms each provided with its own
bath room, where hot and cold water was in continuous supply. In the
grounds a wooden pavilion, containing eight small rooms, did good
service for purposes of isolation and, in the latter part of the life of
the Hospital, when surgical cases were more freely admitted, served as
an intermediate location before men were drafted to depot or home for
convalescence.
Having
been in use for several years as a private Sanatorium the Villa Borghese
contained everything necessary for the equipment of a hospital for
medical cases. The Villa was lighted throughout with electricity, whilst
a very complete heating installation ensured equal warmth to all parts
of the Hospital during the severe weather.After
the later decision of the Committee to admit surgical cases the Chambre
Hydropathique, also on the ground floor, was converted into the
operating theatre.
THE MEDICAL AND SURGICAL
GENERAL RECORD.The
Medical Record is of special interest as well as of ample range. The
location of the hospital service entirely in Paris, ruled out at once
cases of injury and illness direct from the trenches. The type of case
allotted by the distributing authorities was thus less of the acute than
of the chronic and often derelict type; cases whose restoration to
health was of as much value per man to the military forces, but often
infinitely more difficult to compass, than that of the acuter casualties
of the battlefield, running a shorter clinical course. Such almost
intractable instances of broken stamina and lost recuperative power,
which are the trouble and perplexity of many military hospitals, were
the staple of the Neuilly medical clinic.
The
hospital, declared and recognised as a homoeopathic hospital, carried on
its daily work on homoeopathic lines, and under the best homoeopathic
auspices, exactly as any similar institution in this country. The
therapeutics were throughout of the school of Hahnemann. The laboratory
findings were made by Paris experts. The nursing sisters were fully
trained and of British qualification; the probationer nurses had
received their preliminary training in British hospitals; all the
nursing staff had bi-lingual qualifications. The internal distribution
of the hospital as rooms of moderate size, mostly en-suite, with smaller
rooms in the detached annexe, was immensely superior to the usual
barrack-like provision of huge wards, and lent itself easily to the
separate treatment of special cases, particularly those of tuberculosis
and typhoid. The latter cases were necessarily those of the later stage,
when fit for transport, and also some with sequelæ of the acute period.
Tuberculosis was always with us, as a distinctive or complicated malady;
and to such an extent as to suggest that tubercle, latent or declared,
was to be reckoned with in most of the chest cases. A good many of the
patients transferred from other hospitals had their transfer papers
marked or sur-marked “Bronchite,” and this, with French
physicians, implies suspected tuberculosis.Analysis
of the hospital records shows that among eighty medical cases, ten of
typhoid or typhoidal sequelæ were treated; none died.Of
acute or chronic disease of the alimentary canal, e.g.,
gastro-enteritis, mucous colitis, etc., there were eight.Nerve
affections of the type of traumatic neuritis, neurasthenia,
sciatica, etc., totaled eight.Cases
of affection of the respiratory organs, including pleuritic
effusion, bronchitis, laryngitis, etc., amounted in all to forty.The
remainder of the medical cases were those of heart disease, renal
disease, acute and chronic rheumatism.Dr.
Hawkes, of Liverpool, for some time Médecin-chef of the Institution,
has, in his abstracts from the case books, given the following which may
be taken as types of cases coming under his care:Case.
(Jules Henillon), coming originally from the Haute-Saone district, was
admitted on March 20th with renal disease. The albuminuria slowly
diminished and ultimately the tests were negative in result. He left
hospital on July 13th and subsequently was reported fit for the front.Case.
(Louis Charcelley) from Tours, having had his right arm amputated on
December 24th, was admitted to Neuilly Hospital on April 22nd, with
respiratory symptoms. Though bacteriological examination of the sputum
was negative as regards the tubercle bacillus, many other
micro-organisms were discovered. The upper part of the right lung was
not above suspicion, and pleuritic sounds were heard at the right base.
He coughed much and suffered from perspirations. The amputation stump
required continuous dressing as the bone was exposed. Under treatment he
greatly improved in condition, gained flesh and the stump healed. Dr.
Hawkes notes that this was a bad case and the patient’s life originally
despaired of.Case.
(Mahomet Fidale), an Algerian soldier, was admitted, who had received
serious nerve wounds in the arm; the nerves of the left arm having been
afterwards sutured (by operation). Notwithstanding this surgical
procedure he had lost much of the power of the left arm. He had already
spent eight months in other hospitals, and remained two months at
Neuilly. During his residence under treatment, the neuralgic pain in the
arm greatly lessened, and he was able to leave for his home in Africa on
July 12th.Case.
(Francois Lafons), wounded in the thigh on August 14th, 1914, had
typhoid on December fifth, followed by phlebitis of the right leg. He
was admitted to Neuilly on March 27th, his leg still splinted. A long
course of medicinal treatment with rest in bed and massage improved his
condition, and on July Ist he was able to appear before the Court of
Appeal, whence, we believe, he was sent home, where further restoration
may be looked for.Cases
such as these do not run a rapid course, they do not allow a brilliant
recovery, and properly belong to the so-called “wastage of
war.” But they constituted most of the hard work, persistent, often
unpromising, of the hospital staff, and the patients were profoundly
grateful for the benefits received.At
first and intentionally the surgery was limited to medical cases having
surgical complications. This required naturally a dressing equipment,
and later, as surgical necessities increased, a full operative
installation was made by the hospital authorities, and a resident House
Surgeon added to the staff. Surgical cases, having regard to the
pronouncement of an eminent authority “that a wounded soldier is
also a sick soldier,” were now admitted to a section of the
hospital beds. The Médecin-chef was at this time alike a homoeopathic
physician of distinction as well as a hospital trained surgeon.
Ultimately the surgical clinic was conducted by a specially appointed
staff surgeon, with the co-operation of his professional colleagues.
The Photo is of Model
T Fords converted to Ambulances and Drivers. It was taken at Ford Motors
in Paris France. It is part of a series that were used by Ford to
Promote its war contributions and also sell vehicles.
Dr.
Hawkes, during his term as Médecin-chef, obtained from Professor
Hartmann (chief of the American Ambulance and a Paris surgeon of
world-wide renown) the courteous assurance that surgical cases,
requiring a highly organised surgical installation, or a special
surgical experience, could be transferred, if necessary, to Professor
Hartmann’s own surgical clinic. Of this professional fraternity
advantage was taken in certain cases whose particular needs required so
wide a range of surgical skill; and special thanks are due alike to Dr.
Hawkes who engineered, and to Professor Hartmann, who co-operated in so
excellent a working arrangement. One case was that of a man with badly
wounded left arm, thigh and leg where gas-gangrene had developed. He was
transferred to Professor Hartmann’s clinic for operation. The case was
beyond surgical relief and the patient died. Other cases of a grave
character similarly dealt with were uniformly fortunate in- their issue.In
the later months of the work at Neuilly the cases were increasingly
surgical. Altogether they totaled one hundred and twenty-two.
Many of these had been operated on at the base hospitals, cases of
fracture having received the requisite surgical first-aid, and bullets
and shrapnel fragments having mostly been extracted. Here the process of
healing merely required watchful safeguarding, and the concussion
injuries and contusions without open wound also required no active
surgical interference.Simple
fractures of the shoulder girdle, arm or legs existed in fourteen
cases. In one the left femur was doubly fractured. Another had a
concurrent lacerated wound of the hip. A third with a fractured humerus
was unfortunately the victim of a fatal typhoid infection.Compound
and complicated fractures numbered in all nine cases. One was that
of shell wound of the left elbow, with double fracture of the bones
constituting the joint. In another of compound fracture of the ribs,
pleurisy was concurrent.Wounds
constituted by far the majority of surgical injuries treated: penetrating
or perforating wounds of the trunk or extremities existed in
fifteen cases. One was an instance of head wound with concussion, who
had been trepanned, and still had defective vision. But the majority
were thoracic injuries with or without penetrated lung.Lacerated
and contused wounds naturally bulked largely, the cases amounting
to twenty-seven. They were mostly due to shrapnel; and chiefly occurred
in the extremities; a few developed gas-gangrene. Of contusions without
open wounds there were six cases.Where
any of these injuries were concurrent the cases have been placed in the
category of the principal lesion.
Neuilly – 1916.LIST OF CASES. – – – – Name – – – –
Malady or Wound.
1—Gueguen,
Joseph—Typhoid.
2—Marty, Maurice—Pleurisy with effusion.
3—Antin, Joseph—Bronchial asthma.
4—Lefrancois, Louis—Effects of exposure.
5—Bosset, Joseph—Bronchial catarrh: Endocarditis
6—Caillon, Alexander—Lesion of jaw.
7—Ploteau, Moise—Bronchitis.
8—Gerondet, Emile—Bronchitis, particularly apical.
9—Jean, Eugene—Enteralgia and Anæmia.
10—Vassia, Jean-Baptiste—Pneumonic sequelæ.
11—Dutriaux, Gaston—Shrapnel injury to foot.
12—Verricles, Paul—Injury to left forearm (shrapnel).
13—Chachuot, Francois–Bacillary infection of right lung; Pleurisy
with effusion.
14—Bapt, Jean—Typhoidal sequelæ.
15—Charpentier, Camille—Tubercular Peritonitis.
16—Lebris, Yves—Tubercular Pleurisy.
17—Bruand, Frederick—Bronchial catarrh.
18—Barracq, Jean—Bronchitis.
19—Paulet, Raoul—Albuminuria and Bronchitis: Syphilis.
20—Charcelley, Louis—Pleurisy; amputation of right arm.
21—Hauchcorne, Celestin—Left Pleurisy; chronic Bronchitis.
22—Lafons, Francois—Bullet wound in left thigh; Typhoid;
Phlebitis.
23—Henillon, Jules—Albuminuria.
24—Warnier, Fernand—Bronchitis; Laryngitis; Neuritis.
25—Postie, Vincent—Bronchitis and Asthma.
26—Castaug, Severn—Typhoid; Gastritis.
27—Crinière, Georges—Gastritis.
28—Ralli, Jean—Bronchitis and Gastritis.
29—Blanc, Aristide—Typhoid sequelæ
30—Fuxo, Diego—Typhoid sequelæ.
31—Peyson, Louis—Influenza and Bronchitis.
32—Ereillard, Pierre—Convalescence from Typhoid and Pleurisy.
33—Lavergne, Louis—Pleurisy: residues.
34—Cassaquet, Leon—Acute rheumatism.
35—Dauphant, Louis—Pleuritic sequelæ.
36—Grandière, Louis—Bronchitis, Dyspepsia, Asthenia.
37—Gaullot, Paul—Pulmonary congestion.
38—Richard,Pierre—Congestion of lungs Hæmoptysis; Pulmonary
congestion of right apex; Tubercular swelling in neck.
39—Rull, François—Convalescent (injury to both legs, sciatic
nerve severed in one).
40—Mijoule, Francois—Wound of jaw.
41—Fidale, Mahomet—Nerve lesions. ,
42—Challet, Alphonse—Suppuration of cervical gland.
43—Pencislelli, Joseph—Chronic Bronchitis; Asthma; ,Hæmoptysis.
44—Valders, Gustav—Rheumatic Neuritis.
45—Gerondet, Emile—Chronic Phthisis.
46—Granville, Jean—Lead Colic.
47—Bauer, Adolph—Pleurisy.
48—Pelletier, Auguste—Chronic Cardiac disease.
49—Brière, Paul—Typhoid.
50—Biencort, Palmyre—Typhoid.
51—Bresquignan, Perrin—Neurasthenia, Shock; Bronchitis.
52—DuBoisguehemeuc—Dilated stomach; Headaches.
53—Sarragosa, Joachim—Chronic Pleurisy.
54—Battais, Pierre—Chronic Bronchitis; Neuralgia, Influenza.
55—Trappeau, Marcel—Laryngeal Phthisis and General Tuberculosis.
56—Gerard, Jules—Bronchitis; Emaciation.
57—Alrig, Guillaume (died)—Acute Phthisis.
58—Chopard, Victor—Acute Rheumatism; Gastritis; Emaciation
59—Lelny, Emile—Acute Bronchitis.
60—Lartiges, Claude—Disease of stomach; Sore throat; Tubercular
Bronchitis.
61—Basset, Pierre—Fracture of forearm. Gas gangrene.
62—Boniface, Octave—Sacro-iliac Osteitis, Abscess
63—Cazard, Emile—Bronchitis.
64—Gregoire, Jules—Phlebitis after Typhoid.
65—Selerne, Joseph—Mucous Colitis.
66—Fourel, Raymond—Bronchitis and Emphysema.
67—Satir, Camille—Bronchitis in right lung summit.
68—Marie, Maurice—Gastro-enteritis.
69—Mallaverne, Pierre—Acute Articular Rheumatism.
70—Carpentier, Alfred—Sequelæ of Tetanus.
71—Catelle, Alcine—Bronchitis.
72—Riou, Theophile—Sciatica.
73—Coste, August—Sciatica.
74—Auger, Eugene—Rheumatism.
75—Dionet, Gerard—Sequelæ of Typhoid Fever; Phlebitis of right
leg.
76—Vittet, Ernest—Sciatica.
77—Bonnardel, Henri—Bullet wound in left hand; Gas asphyxia.
78—Lambert, Réné Jules—Double wound by a ball in the gluteal
region with gas-gangrenous wounds in the calf of leg and in left side of
chest.
79—Raull, Francois—Convalescent after injury to both legs.
Sciatic nerve severed in one.
80—Greffier, Henri—Abdominal pain after operation for
appendicitis.
81—Juste, Claud—After operation for appendicitis; Dental caries.
82—Caemaris, Alexander—Malaria.
83—Lucas, Paul—Acute gout.
84—Lacy, Gustav—Pleurisy and recurring Bronchitis.
85—Frutel, Albert (died)—Bacillary lesion at right apex; Koch’s
bacillus found in the expectoration.
86—Bliss, Marie—Fracture of Radius.
87—Fortas, Casthène—Amputation of arm; Neuritis of stump;
Tuberculosis.
88—Marillies, Ernest—Tuberculosis.
89—Deschambon, Alphonse—Headache.
90—Corneille, Jules—Wound of left shoulder (ball).
91—Vilmouey, Léon—Suspected Tuberculosis.
92—Cauchois, Louis—Shell wound left side.
93—Baque, Isidore—-Injury right chest; Fistula.
94—Averzaw, Paul—Shell wound left foot.
95—Laisne, Alexander—Injury to hip, loins and face.
96—Chirouze, Francois—Bronchitis.
97—Aflalo, Albert—Bronchitis; wound of thigh.
98—Pineteau, Auguste, Lt—Complicated fracture of ribs; Pleurisy.
99—Ducloux (Commandant)—Penetrating wound of head (trephining);
Concussion of brain causing defective vision; Purulent synovitis
of left knee.
100—Merle, Captain—Fracture of humerus (result of bullet wound).
101—Pire, Réné, Lt—Wound of right hand.
102—Tétard, Julien—Bullèt wound lower third left.
103—Becket, Jean—Fracture of shoulder.
104—Logerot, Emile—Wound in right clavicular region.
105—Carrot, Antoine—Wound in left side.
106—Chaumont, Jules—Right leg badly bruised; Fracture of
calcaneum.
107—Plisson, Jules—Splinters of shell in right and left gluteal
muscles.
108—Carrion—Slight wound shoulder blade.
109—Foltier, Auguste—Wound of left leg (healed). Radiograph
showed presence of shell fragnients; (evacuated to American
Ambulance: operation).
110—Marché, Andre—Wound (bullet) of thigh.
111—Gain, Louis—Injury to hand.
112—Beal, Lt—Resection of right knee followed by suppuration.
113—Cone, François—Injury to left thumb.
114—Stab, Henri, Non-Com—Eczema.
115—Laforgue, Jean (Commandant).—Fracture of Tibia
116—Denertie, Lt—Shell wound; Congestion of right lung.
117—Guenlophe, Lt—Amputated left arm; gangrenous stump
118—Puisson,—-Convalescence after operation.
119—Satre, Capt—Fractured left tibia.
120—Questa, Mateo—Bullet wound in both legs.
121—Remond, Henri—Shell wound, lower third right thigh
122—Cortet, Louis—Wound in right thigh (bullet).
123—David, Maurice (died)—Deep wound left hand, left thigh and
left leg; Gas-gangrene; removed to Professor Hartmann’s hospital for
operation.
124—Montrend, Rene—Wound of knee joint.
125—Tête,
Paul—Septic wound left thigh, arm, shoulder.
126—David, iFrançois—Shell wound in hip.
127—Avenel, Armand—Shell wound of left ankle.
128—Etienne, Ernest—Shell wound, multiple contusion.
129—Cedoz, Armand—Superficial wound in head and thorax.
130—Grospalier, Luc—Superficial shell wound.
131—Guillot, Lucien—Multiple contusions.
132—Gauldry, Charles—Contusion of lumbar region and concussion.
133—Toussaint, Alphonse—Contused wound on the left side of head.
134—Dotte, Alphonse—Penetrating shell wound of thigh.
135—Giffet, George—Wound an posterior aspect of thigh.
136—Shiercelin, Alphonse—Multiple contusions.
137—Blanchard,—-Multiple contusions.
138—Boulogne, A—Fragment of projectile in fight lung; another in
thigh.
139—Renaux, Henri—Left inguinal hernia.
140—Sarjas,—-Intestinal colic.
141—Duboc, Louis (died)—Fracture of left humerus; Enteritis.
142—Vaux,—-Multiple wounds.
143—Ousselin, Leon—Wounds of left thigh and right arm.
144—Fouchon—Shrapnel wound of right knee
145—Guichard,—-Fractured jaw (shrapnel)
146—Eymard,—-Wounds in thorax.
147—Ferrier, Gaston—Surface shrapnel wound, in left forearm.
148—Deiahousse,—-Compound fracture of forearm; exit wound
somewhat jagged.
149—Lagirr,—-. Appendicitis; residual condition after operation.
150—Dupuis, Charles—Shell wound in back.
151—Tisseau, Constant—- Fracture of left forearm; lacerated
wound in left hip.
152—Languedoc, Henri—Multiple wounds in both feet.
153—Picot, Jean—Septic wounds in right shoulder
154—Duequencourt, Ferdinand—Frostbite, both feet.
155—Bahn, Auguste—Wounds of both gluteal regions
156—Penifort, Pierre—Shell wounds in left leg.
157—Barcux, Felix—Multiple grenade wounds; contusion of right
shoulder.
158—Wheeler, Baird—Lacerated wound (bullet); Exit wound with
muscular eversion.
159—Bedel, Joinville—Left leg amputated.
160—Kirch, Emile—Amputation of left leg below knee.
161—Geraud, Alfred—Shell wound of the left side in intercostal
region.
162—Glananus,—-Shell, wound on dorsal surface of foot; exit on
sole.
163—Giradeau, Auguste—Bullet wound in left thigh.
164—Bazin,—-Right thigh amputated. Stump having to be removed
through gas gangrene supervening.
165—Bailleux, Etienne—Fracture of left leg.
166—Leroux, Auguste—Penetrating wound of right forearm.
167—Pépy, Pierre—Fracture of left leg.
168—Drouet, Alfred—Compound fracture of left thigh.
169—Sweeny, Gharles, Lt—Perforating wound left side of chest
170—Netteneau, Jules—Old fracture of jaw.
171—Bocquet, Besne—Perforating chest wound.
172—Victourau, Jules—Penetrating wound left thorax.
173—Loison, Ernest—Complicated fracture left tibia.
174—Richard, Emile—Lacerated wound in wall of thorax.
175—Cordier, Henri—Shell wounds of both legs and left hand.
176—Balceinte, Jean—Perforating wound of right thigh.
177—Renolleau, Pierre—Penetrating wounds of shoulders.
178—Eviard, Albert—Shell wound left elbow; double fracture of
joint.
179—Bencher, Pierre—Compound fracture of right thigh.
180—Coic, Louis—Wound of right leg; gas bacillus infection.
181—Garnier, Theophile—Penetrating shell wound of left shoulder.
,
182—Robert, Jean—Penetrating chest wound; fracture of two ribs.
183—Touchot, Ferdinand—Perforating bullet wound of neck.
184—Mouiex, Joseph—Penetrating wound in left thorax.
185—Lucas, Yves—Compound fracture of left humerus.
186—Dehon, Gaston —Hand amputated.
187—Thomas, Maurice—Double fracture of left femur.
188—Rigaud, Auguste—Simple fracture of left~femur.
189—Bosse, Alphonse—Penetrating wound left side
190—Morel, Henri—Wounds both hands, left thigh and leg; wound
left arm; lesion of cubital nerve and paralysis.
191—Schmit, Edouard—Wound in left ribs.
192—Dutreve, Claude—Wound above the heel.
193—Coulon, Louis—Wounds of left hand and back.
194—Michellotte, Jean—Urinary fistula.
195—Colleau, Jean—Fracture of two ribs.
196—Hancement, Guillaume—Contusion of spine; sciatica.
197—Dufay, Albert—Bullet wounds in left buttock and right calf.
198—Charles, Réné—Complicated fracture of left tibia.
199—Moulin, Louis, Lt—Wound in left frontal region
200—Deslandres, Gabriel—Wounded by ball which entered thigh and
injured sciatic nerve.
201—Bourgrois, Joseph—Fracture of humerus.
202—Haillot, André—Wound through right lung.
Neuilly – 1916.THE DAY’S DOINGS (BY A LADY). (Mary
Lambert)
At
8 a.m. the Night Sister and her nurses were relieved and the Sister and
nurses in charge of the patients during the day took over the wards. The
patients had already breakfasted, their beds made and the Night Sister
had given her report of each patient under her care to the Matron.
Preparations were now made for the visit of the doctors and surgeons,
who made their rounds every morning at 9 a.m., when, under their direct
supervision, wounds and burns were dressed, and each patient underwent
careful examination to determine further treatment or, in cases of
convalescence, decision was arrived at as to his ultimate discharge.The
visit of the doctors over, those patients who were able to walk, even if
only on crutches, made their way into the grounds, some to stroll about
under the trees, others to sit and play dominoes or cards, whilst
smoking the inevitable cigarette. The French poilu, not being provided
with a hospital uniform, is a somewhat nondescript, if, at times,
picturesque individual, during his hospital life, clad as he is in a
medley of garments amongst which occasionally it would be difficult to
find anything regimental besides his cap. Those to whom walking was
forbidden or too painful to be indulged in, found a continual pleasure
in the strains of an ancient gramophone, the gift of a kind visitor,
upon which the “Long, Long way to Tipperary,” accompanied by
the poilus, not in French, but in a wonderful jargon in imitation of the
English version, and the Marseillaise, were easy favourites.From
the disposition of the wards, mentioned in another section, those
patients to whom perfect ease and quiet were essential, could indulge to
their heart’s content in silence and rest; their wards being
sufficiently isolated that no sound from the outer world could reach
them. So that one might be listening one moment, to laughter and
merriment in the larger wards, and within a few yards, so to speak,
patients were sleeping or resting quietly in silence broken only by the
warbling of birds or the rustle of wind amongst the trees, whose leaves
gently brushed their windows. Looking up at the hospital when it was
bathed in sunshine, or on wintry days when the trees bowed their
snow-clad branches, there was always an air of well being, always a hum
of contentment or a restfulness that could be felt. In wards where
amputations were slowly healing, men employed themselves for hours
making baskets and nick-nacks of raffia, working steadily and happily
for days to make some little return for the present of a few cigarettes,
some bon-bons perhaps, or only for kindly words spoken from the heart
and taken to the heart, with no material gift to enhance their meaning.Dinner
was served at 11:30; and in the afternoon at 2 p.m., visitors were
allowed, and wives, sisters, sweethearts or friends arrived. For two
hours there was a regular babel of voices in the wards where the cases
of lesser injury and sickness were housed, and the sound of pattering
feet as children ran merrily from bed to bed. In the other Paris
hospitals visits were allowed only once a week, but at Neuilly greater
latitude was given, and every afternoon the poilus might look forward to
a visit from their friends.
Animals
were of course forbidden, but for all that an Algerian succeeded in
secreting his pet, a tiny chinchilla monkey, hidden away-in the ample
folds of his tunic for a fortnight before he was surprised with it on
his shoulder. He was shortly to be discharged to depot and his little
pet (about six inches long and with a long bushy tail) was permitted to
remain with him until that time; so wrapped in a shawl, this charming
little creature with its wee pathetically human face, sat quietly on his
bed, or perched confidingly on his shoulder the while his master worked
assiduously as orderly, stretcher-bearer, or any other work to which he
could (and always willingly) lend his aid.At
six o’clock the doctors paid their second and last visit to the wards,
unless in cases of great sickness or danger, when their visits knew no
definite times and were performed just whenever required, day or night.The
matron also made her final round, and after the evening meal the wards
were prepared for the night. The hospital day begins so early that
“sunset and evening star” finds the patients ready and willing
to settle down. The busy tongue stilled, quietly the hospital lapses
into silence, and once more the night sisters, with their noiseless
tread and hushed voices, resume their duty for another night.One
day especially stood out in the hospital “memories” as of
greater interest and happiness, when two men received the “Croix de
Guerre.” It was customary in Paris for those who are capable of
doing so to attend at “Les Invalides” for their decorations,
and the ceremony was performed in the open-air in the long galleries
surrounding the courtyard where stand the new trophies of war, German
guns, cannon and parts of wrecked aeroplanes and Zeppelins. The two,
patients of Neuilly, however, were unfit for this exertion, and a high
official came to the hospital with his suite to perform the ceremony.
Preparations were begun early in the morning of the “great
day,” and the vestibule and salon leading therefrom were
transformed into a bower of flowers, whilst the tricolour and the Union
Jack were intertwined over the seats apportioned to the visitors. At
three o’clock punctually, the General arrived, and was received by the
assembled staff, medical, nursing and lay. The large doors opening into
the Salon were thrown open, and as many beds as possible had been
brought in and lined the walls, whilst willing hands among the patients
themselves had carried down from other wards those who were unable to
walk, the two poilus to be decorated being amongst those who had to be
brought down in others’ arms.After
a most affecting address, and a recital of the individual acts of valour
which had won their distinctions for the men, the Croix de Guerre was
placed upon their breasts by the General, who taking each man by the
hand addressed him, “In the name of the President of the Republic I
thank you,” then placing his hands on the man’s shoulders and
kissing his cheek, “In the name of France I thank and embrace
you.”The
two heroes, who were perhaps the most retiring and modest men in the
hospital, had done some wonderful acts of valour, one of them having
volunteered to go out under heavy fire to mend telephone wires,
continued his work after his leg was shattered, dragging himself
laboriously over the ground, and being afterwards found unconscious from
pain and loss of blood, but with his work accomplished.After
the ceremony the two men were carried into the dining room where the
General, visitors and staff drank their health, and chatted with them,
the while the other patients were holding high fete in other parts of
the hospital.Speaking
of heroes, perhaps, it will not be amiss to mention here one other of
our Neuilly patients, an American surgeon, “Baird Wheeler,”
serving in the Foreign Legion, and who came to Neuilly suffering from a
lacerated wound in the leg with muscular hernia.
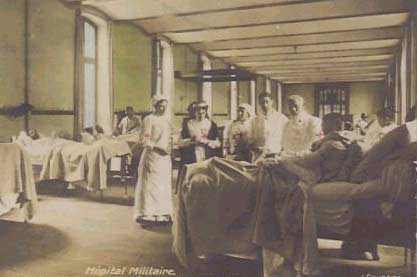
The American
ambulance at Neuilly is doing excellent work for the wounded soldiers.
Many of the nurses are well known society ladies. This photograph shows
some of them with doctors and patients.Dr.
Wheeler, by his cheery good nature endeared himself in an extraordinary
manner to the four other occupants of his room. They could not converse
with him, he knowing no French, and they no English, but for all that
they loved him. He was asked by the American Ambulance to join their
staff, but he was too much of a “sportsman,” he wanted to
fight for France-fought and ultimately gave his life on the battlefield.
Colonel Elkington, in his memories of the Foreign Legion, mentions his
death as a “special loss,” and speaks of him as he appeared to
the writers as a “splendid fellow.”
For
such as these, and for the alleviation of their sufferings the hospital
at Neuilly had its being.
THE FRENCH OFFICIAL
CONTROL OF THE NEUILLY HOSPITAL.The
Anglo-French-American Hospital being under the aegis of the French Red
Cross, two members of this body, Monsieur de Valroger and Monsieur
Basquin, were deputed and voluntarily devoted their time to the
necessary lay administrative detail in connection with the purely
military side of the work at Neuilly. This included keeping the record
of each patient’s Hospital days (necessary in compiling the accounts for
payment of the Capitation grant of Frcs. 2 per diem), arranging for the
reception of patients, and returning them to depot on their discharge.
Dr.
Bernard Arnulphy, who had for several months unweariedly discharged lay
duties as Administrateur, and Professional duties as Consulting
Physician, resigned the former office in November, 1916. Thereafter, at
the instance of the French authorities, Mons. Verde Delisle was
appointed to the vacant post. Dr. Arnulphy remained in office as
Consulting Physician up to the conclusion of the work at Neuilly, and
special record must be made of the continuous and unstinted labour given
by this gentleman, both in lay and professional capacities, in the
interest of the hospital. Particularly at the time of its institution,
and also later in its daily activities, the negotiations and conferences
with the French authorities were mainly conducted by Dr. Arnulphy, and
his close personal relations with Admiral Touchard, the chief of the
Paris Centre of the Croix Rouge Francaise were of great value in solving
many problems of administration.Monsieur
Verdé Delisle on commencing his duties as Administrateur came over to
London once and again, and conferred personally with the Chairman of
Committee on various matters of moment concerning the conduct and
extension of the work at Neuilly.The
services of Monsieur Delisle as an eminent financier were unreservedly
placed, by this gentleman, at the disposal of the Committee, and proved
of conspicuous value in the many-sided negotiations incident to the
conclusion of the activities of the hospital.It
was mainly due to the sound advice of Monsieur Verde Delisle that the
Committee, on reviewing the situation in March 1916, resolved to
recommend the meeting of subscribers to bring this successful work to a
termination.
COMPLETION OF THE ACTIVE LIFE OF THE
HOSPITAL.
During
the active life of the Hospital the French military provision for the
reception of medical and surgical cases had undergone sweeping changes
in the distribution of patients; many of the lesser auxiliary hospitals
had been closed down, and the mass of the cases was being concentrated
in larger institutions or transferred to towns distant from Paris.Concurrently
the Homoeopathic imbalance previously existing in England had become to
some extent rectified. The War Office and Admiralty respectively had
ultimately accepted the offer of beds made by British Homoeopathic
institutions early in the war, and an increasing number of patients from
the Army and the Fleet were being sent to the Homoeopathic hospitals in
England. Thus Homoeopathy had the opportunity of making its public
service known and appreciated in this country. The extra work
necessarily thrown upon medical staffs of the Homoeopathic hospitals, as
well as the number of Homoeopathic doctors called to the colours in the
R.A.M.C. made it increasingly difficult to maintain the requisite
medical staff at the Neuilly Hospital.It
was deemed therefore advisable not to continue the work for an
indefinite period after the original insistent call for its necessity
had lessened. The fact also that the proprietor of the Villa Borghèse
required the use of the building for his own purposes after the 1st
April, thus necessitating a complete change of locale with the attendant
large expense of removing such an institution, was another potent factor
in convincing the Committee of Management of the advisability of
readjusting the situation. This view was confirmed at the Meeting of
Subscribers, held at the London Homoeopathic Hospital on 25th January,
1916, when it was decided that the work of the Hospital might properly
be terminated, and that, if the patients under treatment could be moved,
the hospital should be closed on the 15th March.Beds,
bedding, household linen and effects, hospital requisites of every
description, drugs, dressings and whatever stores were in the hospital
were transferred to the Service de Sante and to the French Red Cross who
received them very gratefully, and expressed much regret at the
termination of the activity of a hospital which had been such a material
and efficient aid to their necessities.The
greatest care and precaution were taken alike by the Matron at Neuilly
and the Committee in London to ensure that every detail of the hospital
equipment provided by the subscribers and friends in England was thus
transferred to the responsible official organizations appointed for the
purpose. The Neuilly Committee considered itself fortunate in that all
the stores, as well as material in actual use which had been entrusted
to its keeping, were thus turned to similar account by the French
official management.Late
in the history of the hospital it had been the wish of the French
military authorities that the whole institution should be reserved for
officers. This suggestion did not meet with the approval of the
Committee of Management, not only on account of the extra expense
entailed, but by reason of the consequent limitation in the grade of
patients admitted for treatment. For this limitation the Committee had
no warrant.Created on 17th April, 1997.
Dr. M. Geoffrey
Miller
The World War I Document ArchivesThis Section of WWI/WWW is concerned with all Medical
aspects, Military and Civilian, of the Great War.Dr. M. Geoffrey Miller
Dr.
Miller, MB.BS. (Lond), MRCP. (Lond), FACRM., FFRM, RACP., MRCS.(Eng).,
is a consultant physician in internal, cardiological and rehabilitation
medicine, practicing in Sydney, Australia, and has a particular interest
in the medical problems of war veterans.He
has had a longtime interest in medical and military history, commencing
the study of naval history whilst a medical student in order to maintain
his sanity. Current projects include research into the death of Manfred
von Richthofen, the medical aspects of Gas Warfare and shell shock.Dr Miller can be contacted for information or
correspondence at: gmiller6@bigpond.net.auCopyright © Dr
M. Geoffrey Miller 1999
Remerciements à la Mairie de Neuilly et H.I. pour
les photos.





